By Yugvender Shrivastav (YU-G) | yugvendershrivastav.com
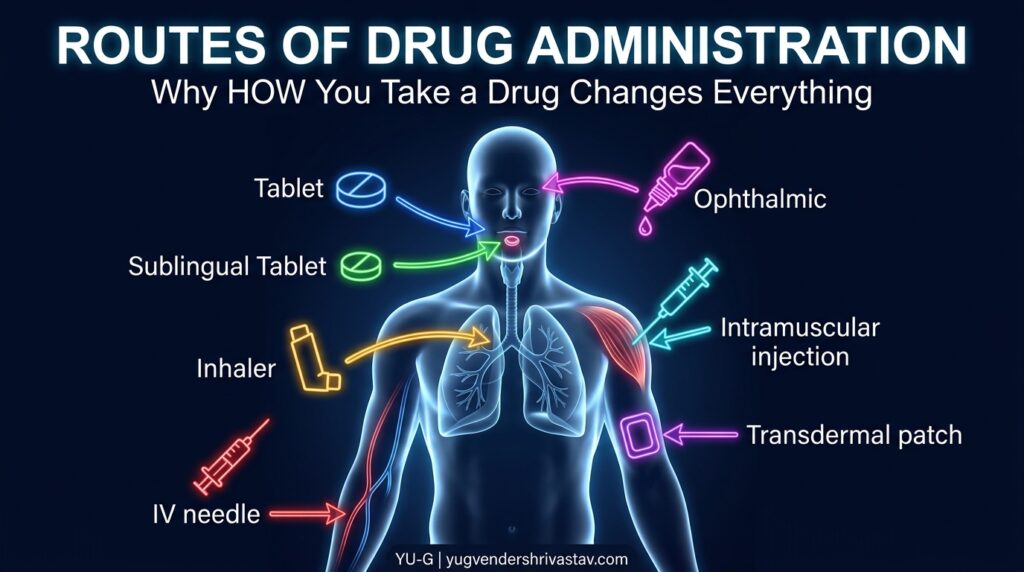
Routes of Administration in One Line: The route of drug administration is the path by which a drug enters the body — and it directly determines how fast the drug works, how much of it reaches the target, and how long its effect lasts.
Same Drug. Different Route. Completely Different Story.
Here’s something that should make you think:
Morphine given orally and morphine given intravenously are the same molecule. Same drug. Same dose on paper.
But IV morphine hits within seconds. Oral morphine takes 30–90 minutes. The IV dose needed is a fraction of the oral dose to produce the same effect. And the risk of overdose with IV is dramatically higher.
Nothing about the drug changed. Only how it entered the body changed.
That’s the power of the route of administration. It’s not a minor detail on a prescription — it’s a fundamental pharmacokinetic variable that shapes everything about how a drug behaves.
If pharmacology is the science of drugs, then routes of administration are the delivery architecture of that science.
Let’s map the entire landscape.
What Is a Route of Administration?
Route of administration (definition): The path or method by which a drug is introduced into the body to reach its site of absorption and, ultimately, its target site of action.
Choosing the right route isn’t arbitrary. It depends on:
- The drug’s physical and chemical properties — Is it stable in stomach acid? Can it cross mucous membranes? Is it water-soluble?
- The desired speed of onset — Emergency? Minutes matter. Chronic therapy? Slow and steady wins.
- The site of action — Local effect (skin, eye) or systemic effect (whole body)?
- Patient factors — Conscious or unconscious? Cooperative or not? Able to swallow?
- The drug’s first-pass metabolism — Will the liver destroy it before it reaches circulation?
Routes are broadly divided into two categories:
| Category | Meaning |
|---|---|
| Local (Topical) | Drug acts at the site of application; minimal systemic absorption |
| Systemic | Drug enters the bloodstream and is distributed throughout the body |
Systemic routes are further divided into enteral (via the GI tract) and parenteral (bypassing the GI tract).
WHO — Medicines Administration Guidelines
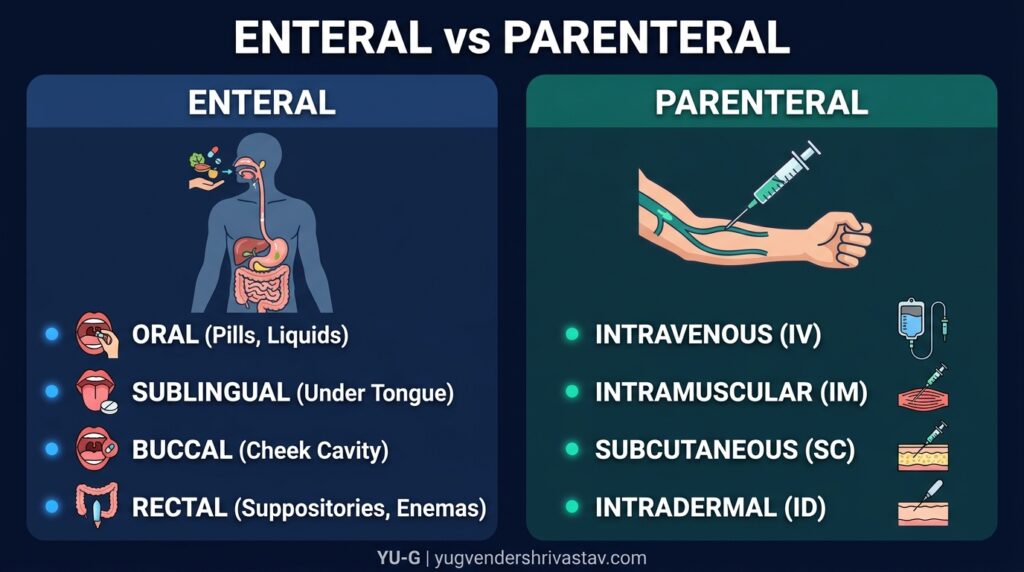
ENTERAL ROUTES — Through the Gastrointestinal Tract
Enteral route (definition): Any route of drug administration that involves passage through the gastrointestinal (GI) tract — including oral, sublingual, buccal, and rectal routes.
💊 1. Oral Route
The oral route is the most common, most convenient, and most preferred route of drug administration in the world.
The drug is swallowed, travels through the GI tract, and is absorbed — primarily in the small intestine (due to its large surface area, rich blood supply, and slightly alkaline pH favorable for many drug molecules).
Advantages:
- Safest and most convenient — self-administered, no needles
- Cost-effective; easy to manufacture (tablets, capsules, syrups, suspensions)
- Suitable for long-term and chronic therapy
- Can be reversed — if overdose is caught early, gastric lavage or activated charcoal can limit absorption
Disadvantages:
- Slow onset — absorption takes time; not suitable for emergencies
- First-pass metabolism — the absorbed drug travels via the portal vein directly to the liver before reaching systemic circulation. The liver may metabolize a significant fraction of the drug before it ever reaches its target. This dramatically reduces bioavailability for some drugs.
- Acid/enzyme degradation — drugs unstable in stomach acid (e.g., insulin, penicillin G) are destroyed before absorption
- Requires patient cooperation — unconscious or vomiting patients cannot take oral drugs
- Erratic absorption — food, GI motility, and disease states affect absorption unpredictably
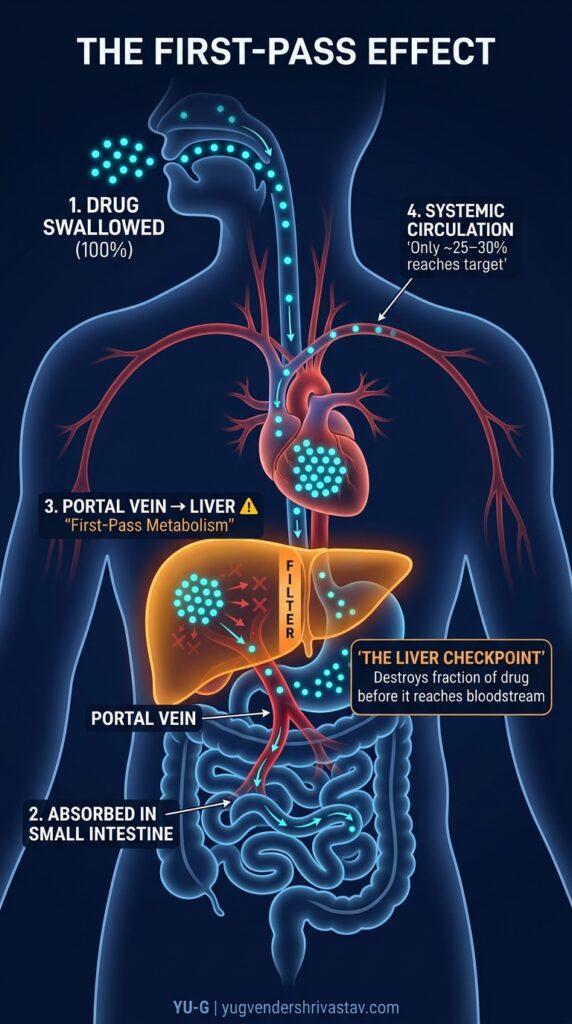
The First-Pass Effect (Explained): Imagine you’re trying to send 100 soldiers (drug molecules) from the GI tract to the battlefield (target organ). But before they can reach the battlefield, they have to pass through a strict checkpoint — the liver. The liver pulls out and destroys 60 soldiers before letting the rest through. Only 40 soldiers make it. That’s the first-pass effect — and it’s why oral bioavailability for drugs like morphine (~25%), propranolol (~30%), and lidocaine (~3%) is so low. You have to give a much higher oral dose to compensate.
Examples of oral drugs: Paracetamol, Metformin, Amoxicillin, Omeprazole, Amlodipine
👅 2. Sublingual Route (SL)
Sublingual (definition): Administration of a drug by placing it under the tongue, where it dissolves and is absorbed directly through the highly vascular sublingual mucosa into the systemic circulation.
The area under your tongue is richly supplied with blood vessels and is highly permeable. Drugs placed here bypass the GI tract AND the liver entirely — going directly into the bloodstream.
Result: Rapid onset (1–3 minutes), high bioavailability, no first-pass metabolism.
This is exactly why sublingual nitroglycerin is the first-line emergency treatment for angina (chest pain). When a patient is clutching their chest in pain, you need that drug working in under 2 minutes — not 45 minutes from now.
Advantages:
- Rapid onset — near-parenteral speed
- Bypasses first-pass metabolism completely
- Drug not degraded by gastric acid or enzymes
- Easy to use; patient can self-administer
Disadvantages:
- Only suitable for small doses of potent, lipid-soluble drugs
- Drug must not be swallowed (defeats the purpose)
- Limited drug options — not all molecules can be absorbed sublingually
- Taste issues; mucosal irritation with some drugs
Examples: Nitroglycerin (GTN), Buprenorphine, Ergotamine, some Fentanyl formulations
3. Buccal Route
Buccal (definition): Drug administration by placing the formulation between the gum and the inner cheek, where it is absorbed through the buccal mucosa.
Similar in principle to sublingual — drug is absorbed through oral mucosa, bypassing first-pass metabolism. Slower than sublingual but provides more sustained absorption.
Examples: Buccal testosterone tablets, some buprenorphine formulations, nicotine gum (partial buccal absorption)
🚽 4. Rectal Route (PR — Per Rectum)
The drug is administered as a suppository, enema, or gel into the rectum.
When is this useful?
- Patient is unconscious, vomiting, or unable to swallow
- Drugs that irritate the gastric mucosa
- Pediatric patients who refuse oral medication
- Local rectal conditions (hemorrhoids, inflammatory bowel disease)
Pharmacokinetic note: Rectal absorption partially bypasses the liver. The lower and middle rectal veins drain directly into the inferior vena cava (bypassing portal circulation), while the upper rectal vein drains into the portal vein. So first-pass effect is reduced but not eliminated — bioavailability is intermediate.
Disadvantages: Irregular, unpredictable absorption; patient discomfort and poor compliance; rectal irritation.
Examples: Diazepam suppositories (status epilepticus in children), Paracetamol suppositories, Mesalazine enemas (ulcerative colitis), Misoprostol
PARENTERAL ROUTES — Bypassing the GI Tract
Parenteral route (definition): Any route of drug administration that bypasses the gastrointestinal tract, typically involving injection or infusion — offering more precise, faster, and more complete drug delivery.
“Parenteral” comes from the Greek para (beside) + enteron (intestine) — literally, “beside the intestine.”
Parenteral routes are used when:
- Rapid action is essential
- The drug is destroyed by the GI tract
- The patient cannot take anything orally
- Precise, controlled plasma levels are needed
- Very large doses are required
💉 5. Intravenous Route (IV)
The drug is injected directly into a vein, entering systemic circulation instantly.
This is the gold standard of all parenteral routes — and the most powerful tool in emergency and critical care medicine.
Advantages:
- Immediate onset — drug reaches blood instantly; effect begins in seconds
- 100% bioavailability — by definition; the drug IS in the bloodstream
- Precise, controllable — dose can be titrated in real time (e.g., IV morphine for pain)
- Large volumes possible — IV fluids, blood products, chemotherapy infusions
- Only option for drugs insoluble in tissue (must be in solution)
- Suitable for unconscious, critically ill, or surgical patients
Disadvantages:
- Irreversibility — once injected, you cannot take it back. Errors are potentially fatal.
- Requires trained personnel and sterile technique
- Risk of infection, phlebitis (vein inflammation), air embolism, extravasation
- Painful; requires IV access
- Cannot use suspensions or oily preparations IV (risk of embolism)
Advanced insight: IV drugs can be given as a bolus (single rapid injection — for immediate effect) or as an infusion (slow, continuous drip — for sustained, controlled plasma levels). The choice between bolus and infusion is itself a pharmacokinetic decision — it determines the peak plasma concentration, the time-concentration profile, and the risk of toxicity. This principle is critical in ICU management of drugs like heparin, insulin, and vasopressors.
Examples: Morphine (emergency analgesia), Adrenaline/Epinephrine (anaphylaxis), IV Antibiotics (sepsis), Chemotherapy agents, IV Fluids
💪 6. Intramuscular Route (IM)
The drug is injected into a muscle — typically the deltoid (upper arm), gluteus maximus (buttock), or vastus lateralis (thigh).
Muscles have a rich blood supply. Drug is absorbed from muscle tissue into capillaries and enters systemic circulation.
Onset: 10–30 minutes (faster than oral, slower than IV)
Advantages:
- Faster and more reliable than oral
- Suitable for oily preparations and depot formulations
- Does not require IV access
- More practical in field/emergency settings than IV
Disadvantages:
- Painful injection
- Cannot inject large volumes (maximum ~5 mL per site)
- Absorption can be unreliable in poor circulation (shock, peripheral vascular disease)
- Risk of nerve injury, abscess, hematoma
Depot Injections: Some IM formulations are specifically designed for slow, sustained release over weeks or months — called depot or long-acting injectable (LAI) formulations. Example: Haloperidol decanoate (antipsychotic) given monthly IM — ensures medication adherence in patients with schizophrenia who might not reliably take daily oral medication. This is a pharmacokinetic strategy with direct clinical implications.
Examples: Vaccines (most), Diclofenac IM, Insulin (sometimes), Haloperidol depot, Benzathine Penicillin
🩺 7. Subcutaneous Route (SC / SQ)
The drug is injected into the subcutaneous tissue — the layer of fat and connective tissue just beneath the skin.
Blood supply here is less dense than muscle, so absorption is slower and more sustained than IM — which is often exactly what’s needed.
Classic example: Insulin. Diabetic patients inject insulin subcutaneously because it provides steady, controlled absorption over hours — mimicking the gradual action of natural insulin.
Advantages:
- Sustained, steady absorption — ideal for drugs needing prolonged action
- Suitable for self-administration (insulin pens, heparin syringes)
- Less painful than IM in many cases
Disadvantages:
- Slow onset — not for emergencies
- Limited volume (~1–2 mL)
- Lipodystrophy (fat tissue damage) with repeated injections at same site
- Absorption affected by tissue perfusion (reduced in shock)
Examples: Insulin, Low molecular weight heparin (Enoxaparin), Adrenaline (in mild allergic reactions), Some vaccines, Biologics (e.g., Adalimumab for rheumatoid arthritis)
🧠 8. Intradermal Route (ID)
The drug is injected into the dermis — the layer of skin just below the epidermis.
Volume is extremely small (~0.1 mL). Absorption is minimal and slow — which is not a disadvantage here but a deliberate feature.
Primary uses:
- Diagnostic testing — Tuberculin skin test (Mantoux test) for TB detection; allergy skin tests
- Vaccines — BCG vaccine (TB), intradermal flu vaccines in some countries
Examples: Mantoux test (PPD), BCG vaccine, Allergy testing
🧬 9. Intrathecal / Spinal Route
Intrathecal (definition): Injection of a drug directly into the subarachnoid space of the spinal canal, where it enters the cerebrospinal fluid (CSF) and reaches the spinal cord or brain directly.
This route exists because of one major challenge: the blood-brain barrier (BBB) — a highly selective barrier that prevents most drugs from entering the central nervous system from the bloodstream.
For drugs that need to act in the CNS but cannot cross the BBB, intrathecal delivery is the solution.
Uses:
- Spinal anesthesia — bupivacaine, lignocaine (for surgeries below the waist)
- Cancer pain management — intrathecal opioids or ziconotide
- Meningitis treatment — antibiotics that don’t cross the BBB (e.g., amphotericin B for fungal meningitis)
- Spasticity — intrathecal baclofen for severe spasticity
Risk: Serious procedure — infection (meningitis), CSF leak, headache, neurological damage if done incorrectly.
🫁 10. Intraosseous Route (IO)
Direct injection into the bone marrow cavity — typically the tibia or sternum.
Bone marrow has a rich vascular network that drains directly into systemic circulation. When IV access is impossible (collapsed veins in shock, cardiac arrest), IO provides an equally fast alternative.
Used in: Pediatric emergencies, cardiac arrest, mass casualty events — when IV access fails and every second counts.
Onset: Nearly identical to IV.
LOCAL / TOPICAL ROUTES
These routes deliver drugs to a specific local site — minimizing systemic absorption and systemic side effects.
🖐️ 11. Topical / Cutaneous Route
Drug is applied to the skin surface for local effect.
Examples: Antifungal creams (clotrimazole), Hydrocortisone cream, Acne gels (benzoyl peroxide, tretinoin), Antiseptics
Key principle: The intact skin is an excellent barrier. Most topically applied drugs stay local — which is the goal. Damaged, inflamed, or abraded skin absorbs significantly more drug, increasing systemic exposure unintentionally.
🩹 12. Transdermal Route (TDD)
Transdermal (definition): Drug delivery through intact skin via a patch or gel system, providing slow, sustained absorption into the systemic circulation over hours to days.
This is different from topical — transdermal drugs are intended for systemic effect. The skin acts as a controlled-release reservoir.
Advantages:
- Avoids first-pass metabolism entirely
- Sustained, steady plasma levels — no peaks and troughs
- Convenient — once-daily or multi-day patches
- Non-invasive; easy to discontinue
Disadvantages:
- Only suitable for highly potent, lipid-soluble drugs in small doses
- Slow onset — not for acute conditions
- Skin irritation, contact dermatitis
- Variable absorption based on skin condition, age, body site
Examples: Nitroglycerin patch (angina prophylaxis), Fentanyl patch (chronic cancer pain), Nicotine patch (smoking cessation), Testosterone gel, Scopolamine patch (motion sickness), Clonidine patch
👁️ 13. Ophthalmic Route
Drug applied directly to the eye — as drops, ointments, or gels — for local effect on the conjunctiva, cornea, or anterior chamber.
Key challenge: Nasolacrimal drainage. Most of the applied drop (up to 70–80%) drains away through the nasolacrimal duct into the nose and throat within seconds — meaning very little drug is actually absorbed into the eye. Applying gentle pressure to the inner corner of the eye after instillation (nasolacrimal occlusion) significantly improves absorption.
Systemic absorption through nasal mucosa can occur and cause systemic side effects. Classic example: Timolol eye drops (for glaucoma) can cause bradycardia and bronchospasm in susceptible patients through systemic absorption — a critical counseling point.
Examples: Timolol (glaucoma), Ciprofloxacin drops (eye infections), Dexamethasone drops (inflammation), Latanoprost (glaucoma)
👃 14. Intranasal Route
Drug administered into the nasal cavity — absorbed through the nasal mucosa.
The nasal mucosa is highly vascular and permeable. Drugs absorbed here bypass first-pass metabolism and reach systemic circulation quickly.
Also used for CNS delivery: The olfactory region of the nasal cavity has a direct anatomical connection to the brain — the nose-to-brain pathway — making intranasal delivery an emerging route for CNS drugs that struggle to cross the BBB.
Examples: Intranasal corticosteroids (allergic rhinitis — Fluticasone, Budesonide), Sumatriptan nasal spray (migraine), Desmopressin nasal spray (diabetes insipidus), Naloxone nasal spray (opioid overdose reversal — a life-saving application), Ketamine intranasal (emerging for depression)
🫁 15. Inhalational Route
Drug is inhaled as a gas, aerosol, or fine powder and absorbed through the large surface area of the lungs (~70 m² — roughly the size of a tennis court).
The pulmonary alveoli have an extremely thin membrane (~0.5 μm) and massive blood flow — making inhalation one of the fastest non-IV routes.
Two purposes:
A) Local pulmonary effect:
- Bronchodilators (Salbutamol, Ipratropium) — directly relax airway smooth muscle in asthma/COPD
- Inhaled corticosteroids (Budesonide, Fluticasone) — reduce airway inflammation locally
B) Systemic effect via lungs:
- General anesthetic gases (Sevoflurane, Isoflurane) — inhaled and distributed systemically via blood
- Nicotine from smoking — absorbed through lungs into blood, reaches brain in ~7 seconds
Advantages: Rapid onset, direct delivery to target (for respiratory drugs), lower doses needed, minimal systemic side effects for local drugs.
Disadvantages: Requires correct inhaler technique (a major real-world challenge — studies show over 70% of patients use inhalers incorrectly), not suitable for all drugs, variable lung deposition.
Pharmacy students: Inhaler technique counseling is one of your most impactful clinical contributions. A patient using a correct drug with wrong technique gets almost no benefit. Always demonstrate, then ask the patient to demonstrate back.
🦷 16. Other Specialized Routes
| Route | Description | Example |
|---|---|---|
| Intra-articular | Injection into a joint space | Corticosteroid injection for arthritis |
| Intracardiac | Injection directly into the heart | Adrenaline in cardiac arrest (rarely used now) |
| Intravaginal | Drug placed in vagina | Clotrimazole pessary (vaginal thrush), Misoprostol |
| Intraperitoneal | Into the peritoneal cavity | Some chemotherapy (ovarian cancer), dialysis |
| Intravesical | Into the urinary bladder | BCG therapy for bladder cancer |
Comparing All Routes at a Glance
| Route | Onset | Bioavailability | First-Pass? | Self-Admin? | Emergency Use? |
|---|---|---|---|---|---|
| Oral | Slow (30–90 min) | Variable | Yes | ✅ | ❌ |
| Sublingual | Rapid (1–3 min) | High | No | ✅ | ✅ |
| Buccal | Moderate | High | No | ✅ | ❌ |
| Rectal | Variable | Partial bypass | Partial | ✅ | Occasionally |
| IV | Immediate (seconds) | 100% | No | ❌ | ✅✅ |
| IM | Moderate (10–30 min) | High | No | Sometimes | ✅ |
| SC | Slow-moderate | High | No | ✅ | ❌ |
| Intradermal | Minimal systemic | Very low | No | ❌ | ❌ |
| Intrathecal | Immediate (CNS) | Direct CNS | No | ❌ | Occasionally |
| Transdermal | Very slow (hours) | Variable | No | ✅ | ❌ |
| Inhalation | Rapid (minutes) | High (pulmonary) | No | ✅ | ✅ |
| Intranasal | Rapid | Moderate-High | No | ✅ | ✅ |
The Elevator Analogy — Why Route Selection Is a Clinical Decision
Think of getting a drug to its target like getting a person to the 10th floor of a building:
- Oral route = Taking the stairs. Safe, accessible, but slow. And there’s a security guard on the 3rd floor (the liver) who stops some people from going further.
- Sublingual/Transdermal = Taking a side entrance that bypasses the security guard entirely. Faster, cleaner access — but only certain people (drugs) can use this entrance.
- IV route = Being teleported directly to the 10th floor. Instant. No barriers. But if you teleport the wrong person (wrong drug, wrong dose) — there’s no way to bring them back.
- Inhalation = A fast elevator that opens only on respiratory floors — perfect if that’s where you’re going.
- Intrathecal = A private, restricted-access elevator to the brain suite — used only when nothing else can get there.
The drug is the same person. The route determines the journey.
Why Pharmacists Must Master This Topic
Routes of administration is not just pharmacokinetics theory — it has direct, daily clinical consequences:
- A patient switched from IV to oral morphine needs a dramatically higher oral dose to maintain the same analgesia — because of first-pass metabolism. Missing this = undertreated pain.
- A patient using a nitroglycerin tablet sublingually who accidentally swallows it gets minimal benefit — the drug is heavily first-pass metabolized orally.
- An asthma patient using an inhaler incorrectly receives a fraction of the intended dose — poor disease control follows.
- Timolol eye drops causing bradycardia in a cardiac patient — systemic absorption through nasal mucosa. A pharmacist who knows this can flag the interaction.
- Depot antipsychotic injections for adherence — understanding this strategy helps you counsel both patients and caregivers.
Route selection and route-specific counseling is where pharmacological knowledge directly saves lives.
Conclusion: The Route Is Part of the Drug
In pharmacology, we often focus so much on which drug that we forget to ask how it’s being given. But as you now understand — the route is inseparable from the drug’s performance. Change the route, and you change the onset, the bioavailability, the duration, the risk profile, and the clinical outcome.
The right drug, by the wrong route, at the wrong time — is the wrong treatment.
Master the routes. It will make every other pharmacology concept click faster.
(For the next step in this series, check out: “Pharmacokinetics: ADME Explained Simply” and “Bioavailability and First-Pass Metabolism — Why Oral Drugs Need Higher Doses.”)
✨ Featured Snippet Answer
What are routes of drug administration? Routes of drug administration are the paths by which drugs enter the body. Major routes include oral (swallowed), sublingual (under the tongue), intravenous (into a vein), intramuscular (into muscle), subcutaneous (under skin), inhalational (through the lungs), and transdermal (through the skin). Each route differs in speed of onset, bioavailability, and clinical suitability.
📌 Key Takeaways
- Route of administration directly determines a drug’s onset, bioavailability, duration, and safety profile
- Oral is most convenient but suffers from first-pass metabolism and slow onset
- Sublingual bypasses first-pass completely — that’s why nitroglycerin works in 1–2 minutes
- IV gives 100% bioavailability and instant onset — but errors are irreversible
- Transdermal patches provide slow, sustained systemic delivery without first-pass metabolism
- Inhalation delivers drugs fastest to the lungs — but inhaler technique determines actual dose delivered
- Intrathecal is used for drugs that cannot cross the blood-brain barrier
- Depot IM injections improve adherence by providing weeks to months of drug release from a single dose
- Timolol eye drops can cause systemic side effects — proof that “local” routes are never completely isolated
- Route selection is a clinical decision — not just a delivery convenience
❓ FAQ Section
Q1: What is route of administration in pharmacology? The route of administration is the specific path by which a drug enters the body to reach its site of absorption and action. It determines onset speed, bioavailability, and clinical use. Routes include oral, sublingual, intravenous, intramuscular, subcutaneous, transdermal, inhalational, and others.
Q2: Which route of drug administration is fastest? The intravenous (IV) route is the fastest — drug enters systemic circulation directly, producing effects within seconds. Sublingual and inhalational routes are close alternatives, with onset in 1–5 minutes. Oral is the slowest common route, taking 30–90 minutes for absorption.
Q3: What is first-pass metabolism and which routes avoid it? First-pass metabolism is the liver’s breakdown of an orally absorbed drug before it reaches systemic circulation, significantly reducing bioavailability. Routes that bypass first-pass metabolism include sublingual, buccal, intravenous, intramuscular, subcutaneous, transdermal, inhalational, and intranasal routes.
Q4: Why is sublingual nitroglycerin used for angina and not an oral tablet? Sublingual nitroglycerin bypasses first-pass metabolism and is absorbed directly into the bloodstream through the mouth’s mucosa, producing effects in 1–2 minutes. Oral nitroglycerin is almost completely destroyed by liver first-pass metabolism, making it ineffective for acute angina relief.
Q5: What is a depot injection? A depot injection is an intramuscular formulation designed for slow, sustained drug release over weeks to months from the injection site. It is used primarily for long-acting antipsychotics (e.g., haloperidol decanoate) and contraceptives to improve medication adherence by eliminating the need for daily dosing.
Q6: Why does the IV route have 100% bioavailability? Bioavailability measures the fraction of administered drug that reaches systemic circulation. Since IV drugs are injected directly into the bloodstream, they bypass all absorption barriers — the GI tract, first-pass metabolism, and tissue absorption variability. By definition, 100% of the dose is immediately bioavailable.
Q7: Can eye drops cause systemic side effects? Yes. Eye drops can be absorbed systemically through the nasal mucosa via nasolacrimal drainage. The classic example is timolol eye drops (used for glaucoma) causing bradycardia and bronchospasm in susceptible patients. Applying pressure to the inner corner of the eye after instillation reduces systemic drainage and lowers this risk.